Today’s Supreme Court case hopefully will expose a medical scandal of significant proportions, where minors are subjected to irreversible treatments without sufficient evidence of their benefits and without proper informed consent.
The Court’s ruling (due in June ’25) should call for a desperately needed reevaluation of these practices to ensure the protection and well-being of vulnerable youth.
At least, one can hope, and pray.
Tyler O’Neil is on the case.
It’s hard to wrap your head around just how grotesque it is that many medical associations and the federal government have adopted the idea that it’s healthy to sterilize children in an attempt to “affirm” a stated transgender identity. On Wednesday, the Supreme Court will shed much-needed sunlight on this medical scandal of epic proportions.
Tennessee Solicitor General Matt Rice will explain how activists conspired to flip the Hippocratic Oath on its head. Meanwhile, U.S. Solicitor General Elizabeth Prelogar and American Civil Liberties Union lawyer Chase Strangio—a female who says she identifies as male—will argue that Tennessee’s law banning Frankensteinian medical experiments on kids violates federal law by discriminating on the basis of sex.
The Supreme Court is hearing the case because of this discrimination argument. The U.S. Court of Appeals for the 6th Circuit upheld Tennessee’s law, finding that it doesn’t entail discrimination. But the Biden-Harris administration appealed that decision, and the Supreme Court took up the case—now known as U.S. v. Skrmetti after Jonathan Skrmetti, the Republican attorney general of Tennessee.
Sex is ordinarily determined at fertilization. Our genetic code, either the presence of an XX or XY chromosomal composition, determines our sexed body. With extremely rare disordered exceptions the human organism begins down a road of male or female bodily differentiation.
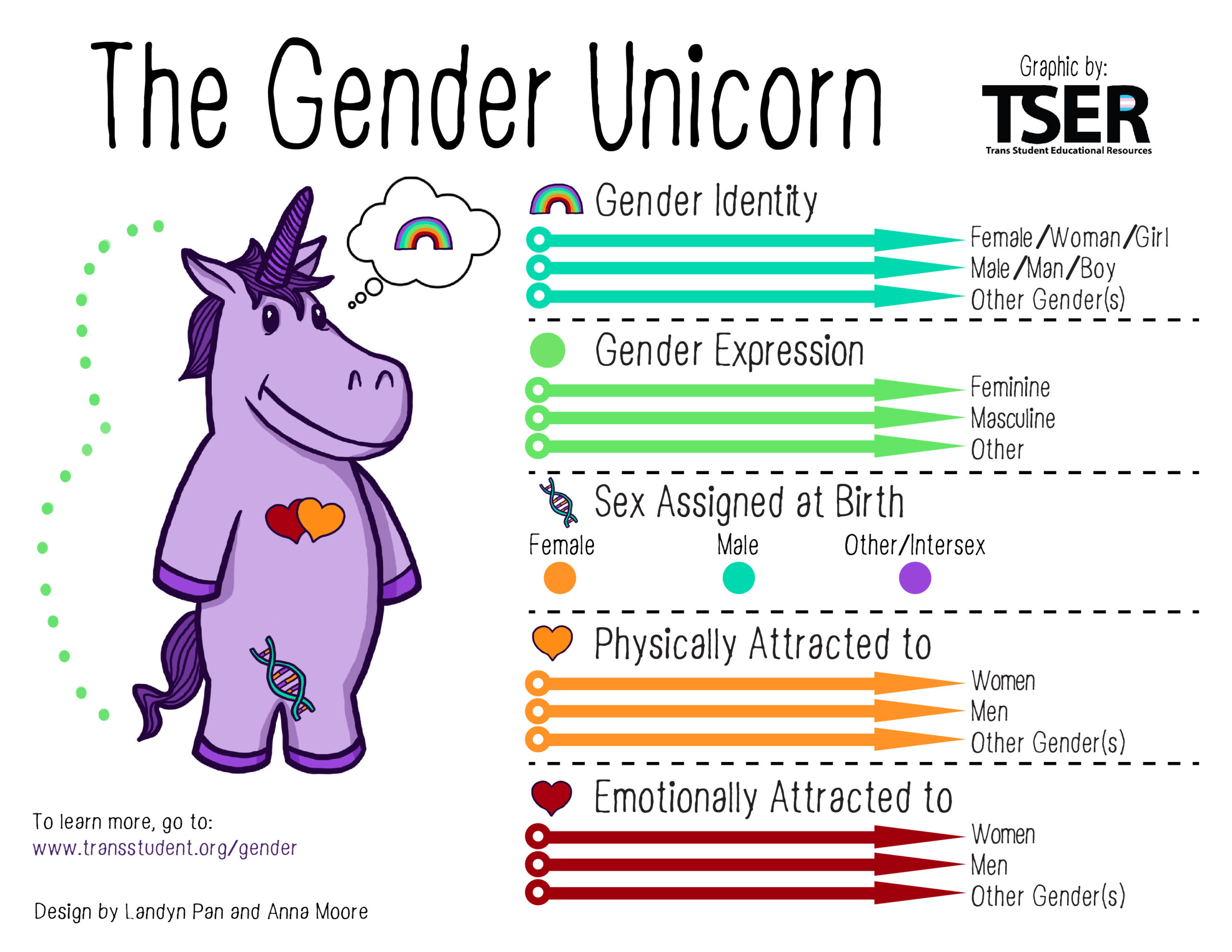
Back to our Gender Unicorn for a moment.
You will notice under the section “Sex Assigned at Birth” a blue dot for “other/intersex.” In the past, what used to be called a “disorder” is now called by many a “difference.” In our decidedly ‘post-modern’ moment, a moment designed to disrupt the very concept of normal or the fact that a natural order exists, we are told by Gender Identity Ideologues that there are a variety of ways that humans can develop. Normal and abnormal categories are obsolete and quite frankly hurtful to those who have developed differently.
Of course any sensitive person is going to treat someone who has one of these rare disorders with love and respect. But we should not ignore the obvious for the purpose of advancing a gender fluid philosophical agenda. Christians can’t do that.
Also, it’s bad science.
Clinics are being pressured to reclassify “Disorders of Sexual Development” as “Differences of Sexual Development.” Some have adopted the new terminology over a concern about stigmatizing people.
But the distinction between order and disorder is operative everywhere in science and medicine. These categories are indispensable for understanding and directing treatments toward human well-being.
Disorders of sexual development (DSDs) occur in roughly one out of every 5,000 births. These disorders can result in ambiguous external genitalia and the incomplete development of reproductive organs. Chromosomal or hormonal defects produce these abnormalities. They are rightly regarded by most medical experts as pathologies in the development and formation of the male and female body. They are exceedingly rare.
But Gender Identity Ideologues use the fact of these rare disorders as a reason for positing a “third sex” “fourth sex” etc., along a spectrum of possibilities. They argue that because of these “differences” the old-fashioned male-female sex binary is obsolete. Some people are just non-binary, they say. As I wrote in a previous post this move is nothing more than the normalization of disorder for the purpose of pushing a gender expansive ideology. (At root this irrationality emanates from an ideology called Queer Theory.)
In 2018 Rev Randall attended a staff seminar at Trent College, entitled “Educate and Celebrate.” He raised an objection when the leader, Elly Barnes, instructed the staff to chant ‘smash heteronormativity.’ For his anti-celebratory concerns he became a marked man at the college.
Barnes’ ideological, dare I say religious, fervor leaves little wiggle room for those like Reverend Randall and myself who believe God made us “male and female.” We don’t believe heteronormativity is oppressive and something to be “smashed.”
***
If you haven’t already added your email to my list, do so and I’ll let you know when the blog is updated.
Dr. Randi Ettner, the chief psychologist at the Chicago Gender Center, describes the standard of care treatment plan promoted by transgender activists, otherwise known as the “Affirmative Care Model“:
• Changes in gender expression and role, consistent with one’s gender identity (also referred to as social role transition).
• Psychotherapy for purposes such as addressing the negative impact of stigma, alleviating internalized transphobia, enhancing social and peer support, improving body image, promoting resiliency, etc.
• Hormone therapy to feminize or masculinize the body.
• Surgery to alter primary and/or secondary sex characteristics.1“Declaration of Randi Ettner, Ph.D., U.S. District Court, Middle District of North Carolina, Case 1:16-cv-236-TDS-JEP, p. 5.”
This plan is often called “transitioning” but some transgender activists regard that term as stigmatizing and inaccurate. From the perspective of the transgender person they are simply engaged in a process of “settling in to themselves” or “coming home” to what they always were inside.2“PFLAG, Our Trans Loved Ones: Questions and Answers for Parents, Families, and Friends of People Who Are Transgender and Gender Expansive (2008, 2015), p. 9, https://www.pflag.org/ourtranslovedones.”
A similar linguistic jujitsu is at work when activists prefer to speak of gender-affirming therapies instead of sex reassignment therapies. (Since when did it become the primary job of doctors to affirm?). For women these affirming therapies mean life-long testosterone, double mastectomies and the creation of a penis (phalloplasty). For men, life-long estrogen, gonadectomy, penectomy, and the creation of a vagina (vaginoplasty). Here are some affirming treatment details:
“Sex reassignment surgeries available to the MTF3male to female transsexual persons consist of gonadectomy, penectomy, and creation of a vagina. The skin of the penis is often inverted to form the wall of the vagina. The scrotum becomes the labia majora. Cosmetic surgery is used to fashion the clitoris and its hood, preserving the neurovascular bundle at the tip of the penis as the neurosensory supply to the clitoris. Most recently, plastic surgeons have developed techniques to fashion labia minora. Endocrinologists should encourage the transsexual person to use their tampon dilators to maintain the depth and width of the vagina throughout the postoperative period until the neovagina is being used frequently in intercourse. Genital sexual responsivity and other aspects of sexual function should be preserved after genital sex reassignment surgery…. Another major effort is the removal of facial and masculine-appearing body hair using either electrolysis or laser treatments. Other feminizing surgery, such as that to feminize the face, is now becoming more popular.
Sex reassignment surgeries available to the FTM4female to male transsexual persons have been less satisfactory. The cosmetic appearance of a neopenis is now very good, but the surgery is multistage and very expensive. Neopenile erection can be achieved only if some mechanical device is imbedded in the penis, e.g. a rod or some inflatable apparatus. Many choose a metaidoioplasty that exteriorizes or brings forward the clitoris and allows for voiding while standing. The scrotum is created from the labia majora with a good cosmetic effect, and testicular prostheses can be implanted. These procedures, as well as oophorectomy, vaginectomy, and complete hysterectomy, are undertaken after a few years of androgen therapy and can be safely performed vaginally with laparoscopy.
The ancillary surgery for the FTM transition that is extremely important is the mastectomy. Breast size only partially regresses with androgen therapy. In adults, discussion about mastectomy usually takes place after androgen therapy is begun. Because some FTM transsexual adolescents present after significant breast development has occurred, mastectomy may be considered before age 18.”5“Hembree et al., “Endocrine Treatment of Transsexual Persons,” 3149.”
Again, like I did in a previous post I must ask, who is engaged in conversion therapy here?
Is it the one who is trying to help a person align their thoughts and feelings with the body they were given at birth or the professional who disregards the body and proposes irreversible radical surgeries combined with life-long hormone treatments in hopes of aligning the outer body with a patient’s inner desires?
Who is the conversion therapist?Gender Identity Ideologues pin that label on those clinicians and pastors who try to help an individual become more comfortable with their immutable biological sex. These concerned professionals and pastors counsel them not to transition away from their birth sex. It’s called Talk Therapy. And it is very effective, especially for children with gender dysphoria. Trans Activists and Gender Identity Ideologues regard these efforts as immoral and professional clinicians are forbidden in some states and other countries from steering individuals toward accepting their birth sex.
Leveling the charge of “conversion therapist” packs quite a rhetorical punch because these therapeutic techniques are said to be just like some of the therapies used in the past to “convert” homosexuals. That’s not true. It’s Talk Therapy! And also, as I’ve said before homosexuals don’t deny their biological sex. This is different. Helping someone align their thoughts and desires with the indisputable facts of their body is not converting them into someone different. Leveling the charge of “conversion therapist” on those professionals or pastors who don’t “affirm” is Orwellian doublespeak. Don’t believe it. And push back. Firmly. Even if you are called a bigot. Do it anyway.
+++
I’m a Classic Christian and regard Gender Ideology as anti-creational to the core. This blog is about “God’s Good Creation.” That’s why I’m writing about Gender Ideology. And “speaking up” as I’m confident Jesus would.
"Have you not read that the one who made them at the beginning 'made them male and female.'" [Matt 19:4]
If you would like more detail on how my Christian worldview informs my understanding of Sex and today’s Gender Ideology please read the following posts.