Podcast Script
My brother had a problem – his heart was not normal. The reason was because he had a rare congenital defect called situs ambiguus. And that meant his major internal organs were abnormally distributed in his body. Most of us have our internal organs in the same location. People with my brother’s condition have kidneys, spleen, pancreas in different locations than the vast majority of us.
Was that merely a difference? Unfortunately. No.
Due to abnormal arrangement of organs in situs ambiguus, orientation across the left-right axis of the body is disrupted early in fetal development, resulting in severely flawed cardiac development and function in 50-80% of cases. My brother, unfortunately, was one of those cases.
My brother only had one atrium and one ventricle. Most of us have 4 chambers in our heart. He had two. Which is why he died of a heart attack at 21 years of age. His birth defect was so bad that he had open heart surgery before the age of two. Most of his life he had this long scar down his midsection where they opened him up as a little boy to repair his birth disorder.
The reason I insist on calling his condition a birth defect or birth disorder and the reason I use the word abnormal to describe his biology. Is because it was. Abnormal. His heart did not function properly. It failed him at a relatively early age. His congenital defect occurs in 1 out of every 10,000 live births.
Now to my larger point. We don’t hesitate to use words like abnormal, and birth defect or disorder when someone is born with half a heart, a heart that cannot do what almost all hearts normally do, pump oxygenated blood throughout the body.
But for some inexplicable reason when the subject turns to our reproductive system or more broadly human sexuality, today, we get very squeamish about using terms like abnormal, or defect, or disorder. Why is that? If someone is born with ambiguous genitalia, you know what that means? Their reproductive system doesn’t work as designed. They have a disorder that is not merely a difference. The system doesn’t work. Now fortunately this won’t lead to an early death. But it will mean their reproductive system is incapable of doing what those systems were designed to do, create life.
The creation of human life and the biological sex of that life, as mentioned in a previous podcast, is determined at fertilization. The Father’s sperm decides. Our genetic code, either the presence of an XX or XY chromosomal composition, determines our sexed body. With extremely rare disordered exceptions the human organism begins down a road of male or female bodily differentiation.
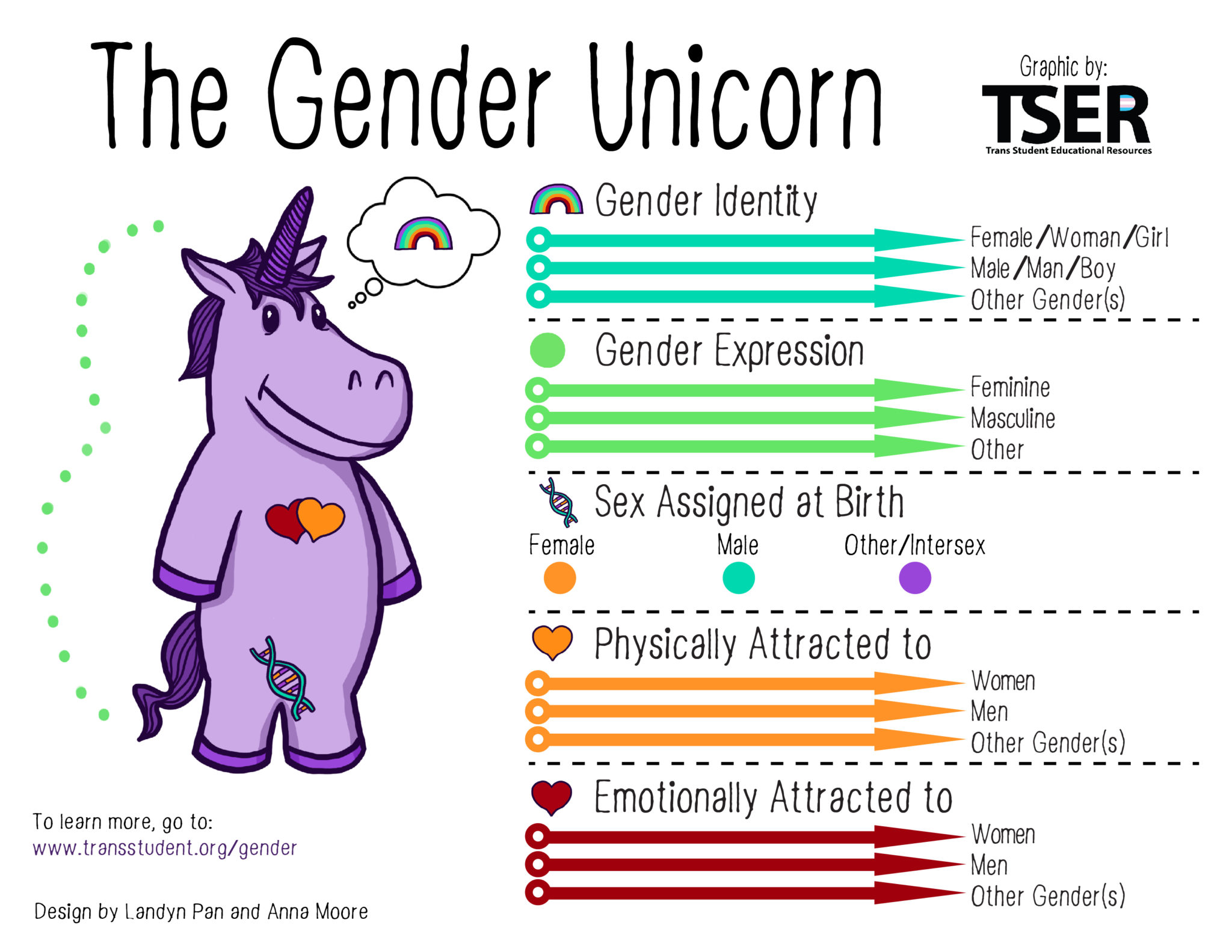
Back to our Gender Unicorn for a moment.
You will notice under the section “Sex Assigned at Birth” a blue dot for “other/intersex.” We need to focus on that.
In the past, what used to be called a “disorder” is now called by many a “difference.”
In our decidedly ‘post-modern’ moment, a moment designed to disrupt the very concept of normal or the fact that a natural order exists, as I believe it does, we are told by Gender Identity Ideologues that there are a variety of ways that humans can develop. Normal and abnormal categories, they say, are obsolete and quite frankly hurtful to those who have developed differently.
Of course any sensitive person is going to treat someone who has one of these rare Intersex disorders with love and respect. But we should not ignore the obvious for the purpose of advancing a gender queer philosophical agenda. Christians can’t do that.
Also, it’s bad science.
Clinics are being pressured to reclassify “Disorders of Sexual Development” as “Differences of Sexual Development.” Some have adopted the new terminology over a concern about stigmatizing people.
But the distinction between order and disorder is operative everywhere in science and medicine. Like with my brother’s disorder. It wasn’t called a “difference”. Though it was. But that would not have been an adequate description. It was accurately called a disorder. These categories of order and disorder are indispensable for understanding and directing treatments toward human well-being.
Disorders of sexual development (DSDs) occur in roughly one out of every 5,000 births. These disorders can result in ambiguous external genitalia and the incomplete development of reproductive organs. Chromosomal or hormonal defects produce these abnormalities. They are rightly regarded by medical experts as pathologies in the development and formation of the male and female body. They are exceedingly rare.
But Gender Identity Ideologues use the fact of these rare disorders as a reason for positing a “third sex” “fourth sex” etc., along a spectrum of possibilities.
In the next few podcasts, I’ll go into more detail about these DSD’s. They argue that because of these “differences” the old-fashioned male-female sex binary is simply obsolete. Some people are just non-binary, they say. As I mentioned in a previous podcast (link below) this move is nothing more than the normalization of disorder for the purpose of pushing a gender expansive ideology. (At root this irrationality emanates from an ideology called Queer Theory.)
Remember the staff trainer, Elly Barnes? In a previous podcast? It was about Rev. Randall. Here’s what I said:
In 2018 Rev Randall attended a staff seminar at Trent College, entitled “Educate and Celebrate.” He raised an objection when the leader, Elly Barnes, instructed the staff to chant ‘smash heteronormativity.’ For his anti-celebratory concerns he became a marked man at the college.
Elly Barnes’ ideological, dare I say religious, fervor leaves little wiggle room for those like Reverend Randall and myself who believe God made us “male and female.” And those are the only options.
Also, we don’t believe heteronormativity is oppressive and something to be “smashed.”
And we understand in the normal course of things that if males and females don’t “get together and ‘share’ genetic material” (a completely unsexy way of stating the matter), then it will result in the extinction of the species.
Why would we want to SMASH that!
Companion Podcasts
+++
Love Refuses To Affirm Confusion